Science
The science of the endocannabinoid system
Ever wondered what the deal is with the endocannabinoid system? Registered Pharmacist Dr Monica Taing explains.

Ever wondered what exactly the deal is with the endocannabinoid system? Registered Pharmacist and clinical cannabis consultant, Dr Monica Taing explains.
The endocannabinoid system [ECS] is a comprehensive and complex homeostatic balancing system with diverse potential therapeutic clinical implications in chronic conditions,” said Monica Taing, PharmD, RPh, at the inaugural meeting of Medical Cannabis: Science, Research and Risks, held at Columbia University [in New York City].

Dr Taing, who is a clinical cannabis consultant specialist for hospital systems and academic medical institutions, spoke to meeting attendees about the pharmacokinetic and pharmacodynamic parameters of various cannabinoids and their effects on homeostasis, chronic disease states, dosing, formulation selection and potential drug interactions.
The role of the ECS in homeostasis
“The ultimate function of the ECS is homeostasis, which is returning balance in the body,” Dr Taing told attendees.
“It is the internal biological balancing mechanism of the body and brain.”
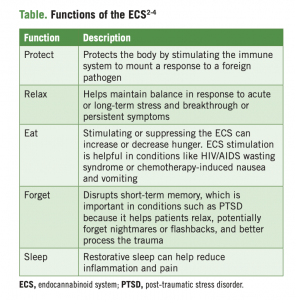
Dr Taing used the acronym PREFS to describe the key functions of the ECS in promoting homeostasis: protect, relax, eat, forget, and sleep.
“The ECS changes as we age,” Dr Taing continued.
“It’s different in every person based not only on age, but also on race, gender, and use of pharmacotherapies that can tip the balance away from or help restore homeostasis.”
Basics of the ECS
Dr Taing cited preclinical data showing that the ECS has a profound effect on stress, anxiety, and depressive states at the pharmacologic, biochemical, and genetic levels.
The fundamental pillars of the ECS, consist of the following:
- CB1 and CB2 receptors are G protein-coupled receptors (upon which a majority of other pharmacologic therapies also impact) produced in the body as a result of human evolution.
- CB1 receptors are ubiquitous throughout the body and are predominantly found in the central nervous system, with a high density in certain areas of the brain (eg, cerebel lum, globus pallidus, hippocampus, and substantia nigra),7 whereas CB2 receptors are mainly limited to the periphery, including the immune system.
- Endocannabinoids: N-arachidonoylethanolamine (anandamide) and 2-arachidonoylglycerol (2-AG) are produced in the body on demand and act as partial agonists at CB1 and CB2 receptors. Activation of these receptors by anandamide and 2-AG has the potential to modulate anxiety/ stress, inflammation, pain perception, and neuropathic pain, among other processes.8,9
- Enzymes produced in the cerebrospinal (uid drive the bio synthesis, degradation, and transport of endocannabinoids and other ligands that act on cannabinoid receptors.10
“It is interesting that CB1 receptors are very minimally, if at all, located in the brainstem,” Dr Taing said.
“This is the pathophysiological reason why it is not physically possible to induce cardiorespiratory depression [solely] with [botanical] cannabis.”
Cannabinoid pharmacology
Delta-9-tetrahydrocannabinol (THC) mimics the effects of anandamide and 2-AG and on CB1 and CB2 receptors, and CBD has multimodal activity at CB1 and CB2 receptors as well as at receptors beyond the ECS, Dr. Taing said.11,12
She uses the lock-and-key metaphor for explaining the complex pharmacology of cannabis to patients, where CB1 and CB2 receptors are the locks and cannabinoids (either endogenously produced or exogenously introduced) are the keys.
Preclinical research suggests that anandamide and 2-AG exhibit local effects on cardiovascular physiology (e.g cardiac contractility, platelet activation, endothelial cell activation) as well as positive effects on other cells that contribute to cardiovascular/ atherosclerotic pathologies (e.g monocytes, macrophages, lymphocytes, neutrophils, and other inflammatory cells).

Monica Taing, PharmD, RPh
“Understanding the activity of CB1 and CB2 receptors in the ECS, ligands (concentration and duration), as well as enzyme synthesis, release, and degradation is needed to understand the diverse therapeutic clinical implications of medical cannabis use in the treatment of chronic conditions,” said Dr Taing.
Additionally, it is important to consider the entourage effect of cannabis, which is the theory that “terpenes, flavonoids and cannabinoids all work together like a symphony.”
“These components all complement each other so that you can get the maximal effect of the plant,” she added.
Terpenes are essential oils that provide aroma and flavour to the plant, whereas (flavonoids provide pigment and potentially antioxidants.
“In practice, I meet patients who are prescribed the synthetic agent dronabinol and say that it didn’t work for them, and this may be because they are not benefiting from the entourage effect,” Dr Taing noted.
This prescription medication also has a narrow indication and may not address all the issues and symptoms that patients with chronic conditions have, she added.
Dosing and safety
THC produces biphasic effects with low doses mimicking the effects of endocannabinoids in reducing hypothalamic–pituitary–adrenal (HPA) axis activity and anxiety, whereas high doses increase HPA axis function and are anxiolytic.
“Biphasic dosing of THC is the pharmacological rationale behind ‘start low, go slow’ dosing for patients, regardless of whether the patient is using an adjustable or inhalation delivery method,” Dr Taing said.
Patient education is particularly important for those taking edible cannabis, as there is a lag in onset of action, and then an extended duration of action compared with inhaled cannabis.
“When the body is starting to digest and metabolise THC, it will convert it to 11-hydroxy THC, a metabolite that is more potent than the original THC and potentially lasts in the body longer,” Dr Taing noted.
“I have seen so many [reported incidents of] patients who took one bite of a cannabis brownie and they didn’t feel any effect after 15 minutes, and then ate the entire brownie and wound up in the emergency room.”
Even in a cannabis-experienced patient, Dr. Taing suggested starting treatment with a product that has less than 10 percent THC. Then she suggests gradually dose titrating by monitoring for efficacy and the emergence of adverse events.
Monitoring for drug interactions also is essential to care.
“We need to monitor patients taking antidepressants or mood stabilizers for changes in terms of how they feel, their effect, their mood, and any short-term and long-term benefits of cannabis in order to manage the dosing of cannabis as well as dosing of the other prescription medications that they are taking,” Dr Taing explained.
“Striking the right balance in terms of dosing also is important for patients with cardiovascular issues, as the risk for an acute cardiovascular attack is increased for one hour after using cannabis,” Dr Taing said.
Additionally, Dr Taing noted that patient counselling for those who are apprehensive is important to ensure that they are in an optimal environment and mindset to obtain benefit from cannabis treatment.
Dr Taing is on the Board of Directors of Doctors for Cannabis Regulation, is the Director of Research and Clinical Education for Minorities for Medical Marijuana and serves as a Medical Science Liaison for 4Front Ventures.
This article was originally published in the American Journal of Endocannabinoid Medicine (AJEM). Find the original article including reference list here
Get the weekly briefing
A round-up of the latest science, regulation and developments across the UK and Europe — in your inbox every week.